Free State Of Louisiana Medication Order Form
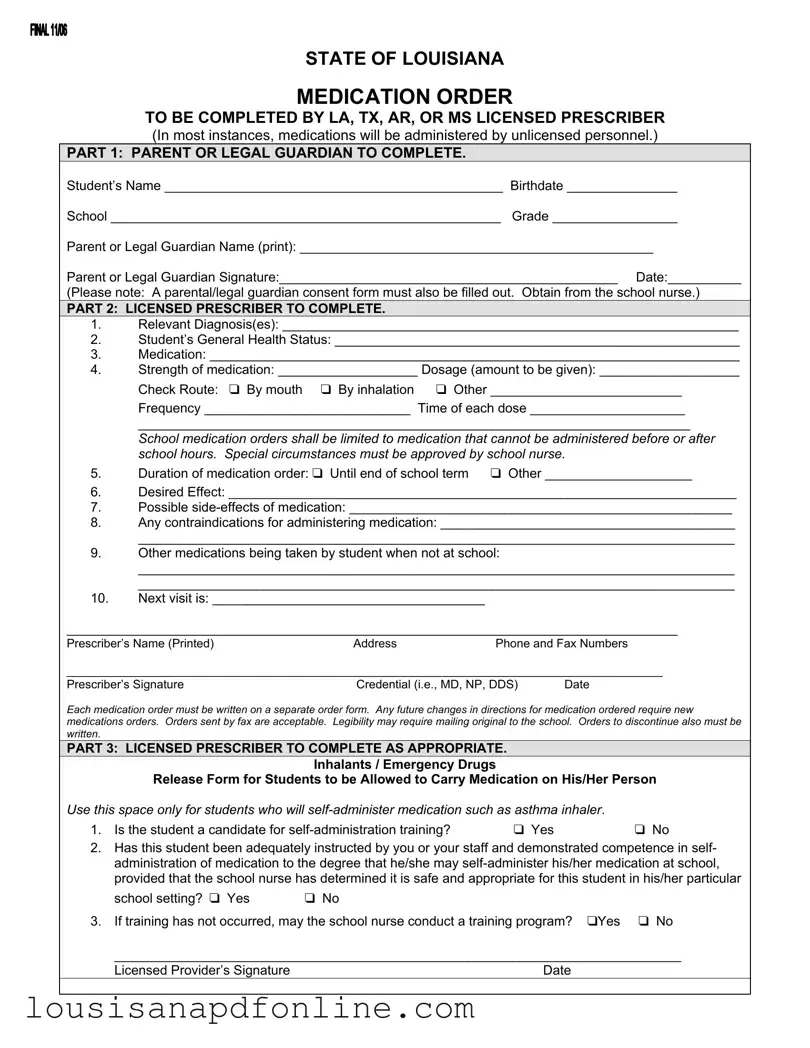
The State of Louisiana Medication Order form is a crucial document designed to ensure that students receive the necessary medications while at school, especially when those medications cannot be administered before or after school hours. This form is divided into three main parts, each serving a specific purpose. The first part requires the parent or legal guardian to provide essential information about the student, including their name, birthdate, school, and grade, as well as obtaining the guardian's signature. Following this, the licensed prescriber completes the second part, detailing the student's relevant diagnosis, general health status, and specific medication information, including dosage, frequency, and administration route. Additionally, this section addresses any potential side effects and contraindications, ensuring that the school staff is well-informed about the student’s health needs. The final part of the form focuses on students who may need to carry their own medications, such as asthma inhalers, allowing for self-administration under certain conditions. Each medication order must be documented on a separate form, and any changes to the medication regimen require new orders, ensuring that the information remains current and accurate for the safety of the student.
Sample - State Of Louisiana Medication Order Form
STATE OF LOUISIANA
MEDICATION ORDER
TO BE COMPLETED BY LA, TX, AR, OR MS LICENSED PRESCRIBER
(In most instances, medications will be administered by unlicensed personnel.)
PART 1: PARENT OR LEGAL GUARDIAN TO COMPLETE.
Student’s Name ______________________________________________ Birthdate _______________
School _____________________________________________________ Grade _________________
Parent or Legal Guardian Name (print): ________________________________________________
Parent or Legal Guardian Signature:______________________________________________ Date:__________
(Please note: A parental/legal guardian consent form must also be filled out. Obtain from the school nurse.)
PART 2: LICENSED PRESCRIBER TO COMPLETE.
1.Relevant Diagnosis(es): ______________________________________________________________
2.Student’s General Health Status: _______________________________________________________
3.Medication: ________________________________________________________________________
4.Strength of medication: ___________________ Dosage (amount to be given): ___________________
|
Check Route: ❑ By mouth ❑ By inhalation ❑ Other __________________________ |
|
|
Frequency ____________________________ Time of each dose _____________________ |
|
|
___________________________________________________________________________ |
|
|
School medication orders shall be limited to medication that cannot be administered before or after |
|
|
school hours. Special circumstances must be approved by school nurse. |
|
5. |
Duration of medication order: ❑ Until end of school term |
❑ Other ____________________ |
6.Desired Effect: _____________________________________________________________________
7.Possible
8.Any contraindications for administering medication: ________________________________________
_________________________________________________________________________________
9.Other medications being taken by student when not at school:
_________________________________________________________________________________
_________________________________________________________________________________
10.Next visit is: _____________________________________
___________________________________________________________________________________
Prescriber’s Name (Printed)AddressPhone and Fax Numbers
__________________________________________________________________________________________
Prescriber’s Signature |
Credential (i.e., MD, NP, DDS) |
Date |
Each medication order must be written on a separate order form. Any future changes in directions for medication ordered require new medications orders. Orders sent by fax are acceptable. Legibility may require mailing original to the school. Orders to discontinue also must be written.
PART 3: LICENSED PRESCRIBER TO COMPLETE AS APPROPRIATE.
Inhalants / Emergency Drugs
Release Form for Students to be Allowed to Carry Medication on His/Her Person
Use this space only for students who will |
|
|
1. Is the student a candidate for |
❑ Yes |
❑ No |
2.Has this student been adequately instructed by you or your staff and demonstrated competence in self- administration of medication to the degree that he/she may
school setting? ❑ Yes ❑ No
3. If training has not occurred, may the school nurse conduct a training program? ❑Yes ❑ No
_____________________________________________________________________________
Licensed Provider’s Signature |
Date |
Form Characteristics
| Fact Name | Details |
|---|---|
| Purpose | The State of Louisiana Medication Order form is designed for licensed prescribers to authorize the administration of medication to students during school hours. |
| Completion Requirements | The form must be completed by a licensed prescriber from Louisiana, Texas, Arkansas, or Mississippi. It requires input from a parent or legal guardian and includes sections for diagnosis, medication details, and health status. |
| Governing Law | This form is governed by Louisiana state law, particularly guidelines related to the administration of medication in schools as outlined in the Louisiana Revised Statutes. |
| Medication Administration | Medications administered at school are typically limited to those that cannot be given before or after school hours. Special circumstances require approval from the school nurse. |
More PDF Forms
Louisiana Application for Military Discount - A simple form to unlock a range of discounts for service members stationed in Louisiana.
Why Did I Receive a Florida Ucc Statement Request Form - The form allows for specifying collateral as diverse as vehicles, accounts receivable, and general intangibles.
Creating a Last Will and Testament is an essential step in ensuring that your wishes are respected after your passing, as it details the distribution of your possessions and appoints an executor to manage your estate. For those looking to draft or understand this important legal document, resources such as UsaLawDocs.com can provide valuable guidance and templates to simplify the process.
Louisiana Disciplinary Board - The form requires a history of any Louisiana court or agency applications for pro hac vice in the last two years, ensuring no abuse of the privilege.