Free Louisiana Medicaid Freedom of Choice List Form
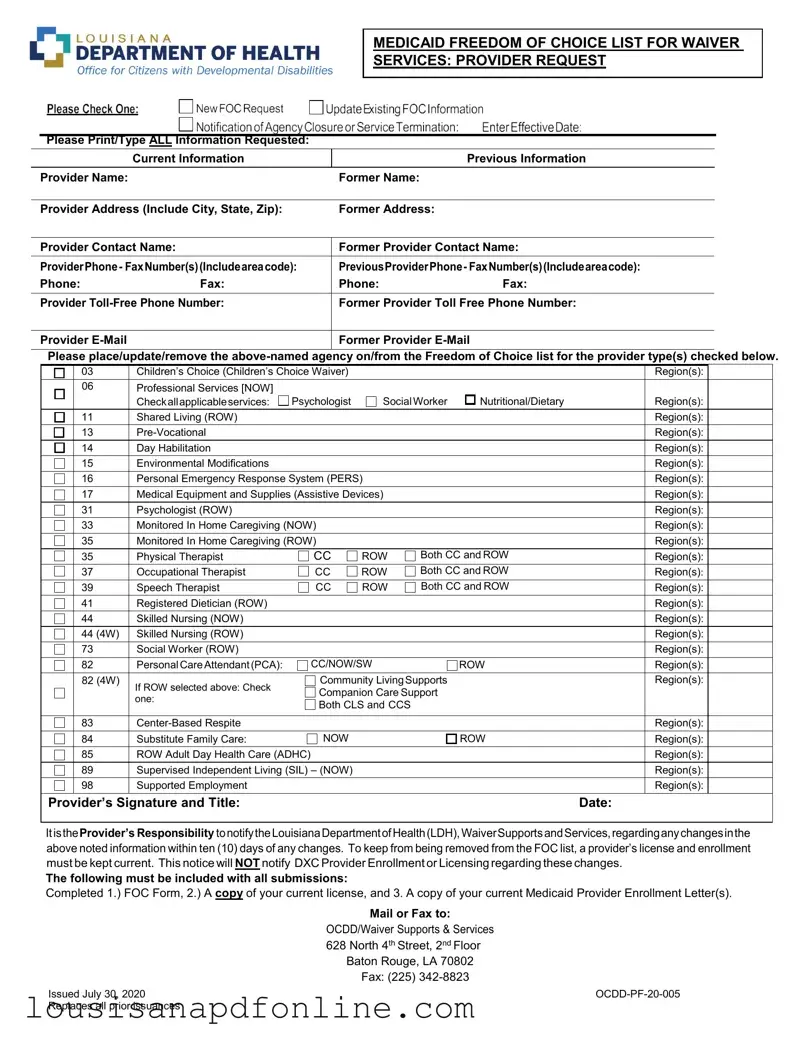
The Louisiana Medicaid Freedom of Choice List form is a crucial document for providers participating in the state's Medicaid waiver services. This form allows providers to request their inclusion or update their status on the Freedom of Choice list, which is essential for ensuring that eligible individuals can access necessary services. It requires comprehensive information, including the provider's current and previous names, addresses, contact details, and specific services offered. Providers must indicate the types of services they provide, such as children's choice waivers, personal emergency response systems, or skilled nursing services, along with the relevant regions they serve. Additionally, the form emphasizes the importance of maintaining up-to-date information, as providers are responsible for notifying the Louisiana Department of Health about any changes within ten days. Failure to do so may result in removal from the Freedom of Choice list, which could significantly impact service accessibility for clients. To complete the process, providers must submit the form along with a copy of their current license and Medicaid Provider Enrollment Letter, ensuring compliance with state regulations. Understanding the nuances of this form is vital for providers to maintain their standing and continue offering essential services to those in need.
Sample - Louisiana Medicaid Freedom of Choice List Form
MEDICAID FREEDOM OF CHOICE LIST FOR WAIVER
SERVICES: PROVIDER REQUEST
Please Print/Type ALL Information Requested:
|
Current Information |
|
Previous Information |
|
|
|
|
Provider Name: |
|
Former Name: |
|
|
|
|
|
Provider Address (Include City, State, Zip): |
Former Address: |
|
|
|
|
||
Provider Contact Name: |
Former Provider Contact Name: |
||
|
|
||
ProviderPhone- FaxNumber(s)(Includeareacode): |
PreviousProviderPhone- FaxNumber(s)(Includeareacode): |
||
Phone: |
Fax: |
Phone: |
Fax: |
|
|
||
Provider |
Former Provider Toll Free Phone Number: |
||
|
|
|
|
Provider |
|
Former Provider |
|
|
|
|
|
Please place/update/remove the
|
03 |
Children’s Choice (Children’s Choice Waiver) |
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
06 |
Professional Services [NOW] |
|
|
|
|
|
|
|
|
|
Checkallapplicableservices: |
Psychologist |
SocialWorker |
Nutritional/Dietary |
|
Region(s): |
|
|
|
11 |
Shared Living (ROW) |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
13 |
|
|
|
|
|
Region(s): |
|
|
|
14 |
Day Habilitation |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
15 |
Environmental Modifications |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
||
|
16 |
Personal Emergency Response System (PERS) |
|
|
|
Region(s): |
|
||
|
|
|
|
|
|
|
|
||
|
17 |
Medical Equipment and Supplies (Assistive Devices) |
|
|
|
Region(s): |
|
||
|
|
|
|
|
|
|
|
|
|
|
31 |
Psychologist (ROW) |
|
|
|
|
|
Region(s): |
|
|
33 |
Monitored In Home Caregiving (NOW) |
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
35 |
Monitored In Home Caregiving (ROW) |
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
35 |
Physical Therapist |
CC |
ROW |
Both CC and ROW |
|
Region(s): |
|
|
|
37 |
Occupational Therapist |
CC |
ROW |
Both CC and ROW |
|
: |
|
|
|
|
|
|
Region(s) |
|
||||
|
39 |
Speech Therapist |
CC |
ROW |
Both CC and ROW |
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
41 |
Registered Dietician (ROW) |
|
|
|
|
|
Region(s): |
|
|
44 |
Skilled Nursing (NOW) |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
44 (4W) |
Skilled Nursing (ROW) |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
73 |
Social Worker (ROW) |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
82 |
Personal CareAttendant(PCA): |
CC/NOW/SW |
|
ROW |
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
||
|
82 (4W) |
If ROW selected above: Check |
Community LivingSupports |
|
|
Region(s): |
|
||
|
|
Companion Care Support |
|
|
|
|
|||
|
|
one: |
|
|
|
|
|||
|
|
Both CLS and CCS |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
83 |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
84 |
Substitute Family Care: |
NOW |
|
|
ROW |
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
85 |
ROW Adult Day Health Care (ADHC) |
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
89 |
Supervised Independent Living (SIL) – (NOW) |
|
|
|
|
Region(s): |
|
|
|
98 |
Supported Employment |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
Provider’s Signature and Title: |
|
|
|
|
Date: |
||||
|
|
|
|
|
|
|
|
|
|
ItistheProvider’s Responsibility tonotifytheLouisianaDepartmentofHealth(LDH),WaiverSupportsandServices,regardinganychangesinthe above noted information within ten (10) days of any changes. To keep from being removed from the FOC list, a provider’s license and enrollment must be kept current. This notice will NOT notify DXC Provider Enrollment or Licensing regarding these changes.
The following must be included with all submissions:
Completed 1.) FOC Form, 2.) A copy of your current license, and 3. A copy of your current Medicaid Provider Enrollment Letter(s).
Mail or Fax to:
OCDD/Waiver Supports & Services
628North 4th Street, 2nd Floor Baton Rouge, LA 70802 Fax: (225)
Issued July 30, 2020 |
|
Replaces all prior issuances |
|
Form Characteristics
| Fact Name | Fact Description |
|---|---|
| Purpose | The Louisiana Medicaid Freedom of Choice List form is used to request the addition, update, or removal of providers from the Freedom of Choice list for waiver services. |
| Required Information | Providers must print or type all requested information, including current and previous names, addresses, and contact details. |
| Provider Types | The form covers various provider types, such as Psychologists, Social Workers, and Personal Care Attendants, among others. |
| Governing Laws | This form operates under Louisiana state laws governing Medicaid waiver services, specifically the Louisiana Department of Health regulations. |
| Submission Requirements | Providers must include a completed Freedom of Choice form, a current license copy, and a current Medicaid Provider Enrollment Letter with their submission. |
| Notification Responsibility | It is the provider's responsibility to notify the Louisiana Department of Health of any changes in information within ten days. |
| Current License | To remain on the Freedom of Choice list, providers must keep their licenses and enrollments current. |
| Submission Methods | Providers can mail or fax their submissions to the Office for Citizens with Developmental Disabilities (OCDD) in Baton Rouge. |
| Issued Date | The current version of the form was issued on July 30, 2020, and replaces all prior issuances. |
More PDF Forms
Louisiana Disciplinary Board - The detailed history of pro hac vice applications prevents potential exploitation of the system by frequently applying out-of-state lawyers.
R-1048 Louisiana 2023 - By requiring employee and employer information, it verifies the legitimacy of the tax exemption claim.
For landlords looking to initiate the eviction process, utilizing a proper form is crucial. The Illinois Notice to Quit can be an effective tool for these purposes. To learn more about how to properly implement this form, refer to the guidelines on the important Notice to Quit requirements.
Inspection Auscultation Percussion Palpation - Assessment of hypoglycemia risks in diabetic patients addresses the potential for sudden medical incapacitation during driving.